1958:009 - MULLACASH MIDDLE, CO. KILDARE, Kildare
County: Kildare
Site name: MULLACASH MIDDLE, CO. KILDARE
Sites and Monuments Record No.: SMR KD024-018
Licence number: E1087
Author: BREANDÁN Ó RÍORDÁIN
Author/Organisation Address: —
Site type: Iron Age and early medieval graves, c. 300 BCc. AD 1200
Period/Dating: —
ITM: E 689144m, N 713483m
Latitude, Longitude (decimal degrees): 53.164371, -6.666870
Introduction
In August 1958 a number of inhumation burials and long cists were discovered during the construction of a fence for the Irish Land Commission at Mullacash Middle between Kilcullen and Naas, Co. Kildare. The ganger in charge reported the find to the Garda Síochána at Naas, who instructed the workmen to remove the bones for examination by the coroner. After this examination was carried out, the site was visited by the Public Health officer, who instructed the workmen to collect the bones and have them reburied in a local interment plot. This was about to be carried out when the site was visited by local historian Mr T.P. Clarke, who saw the stone lining of one of the graves and informed the Gardaí that the site should be reported to the NMI. The site was investigated on 23 August 1958 by Breandán Ó Ríordáin. This report is based on Ó Ríordáin’s excavation report, plans and photographs. The human remains were examined by Laureen Buckley.
Location
The site was in the townland of Mullacash Middle in east County Kildare, close to the border with County Wicklow.48The first edition OS 6in. sheet shows a distinct curvilinear wall, now incorporated into field fences, enclosing most of Mullacash Hill in Mullacash South townland. This may be the remains of an early ecclesiastical enclosure. The remaining portion on the first edition map is very substantial, measuring approximately 260m in diameter. The early medieval site of Killashee is 2km to the north of Mullacash Middle.
Description of site (Pl. 78)
An area 2.8m long by 1.9m wide was chosen for excavation in the part of the field where slabs had been noted by the workmen. Three burials were found: one slab-lined grave, one lintel grave and one unprotected burial overlying the lintel grave. The graves lay between 0.22m and 0.27m below ground level. Miscellaneous bone found on the site was also retained (1958:168).
Grave 1
This burial lay on the lintels of grave 2. Apart from the paved floor (i.e. the roof of the grave underneath) there was no apparent grave structure (Fig. 4.24).
The burial consisted of an extended inhumation of an older adult male (1958:165) and no accompanying artefacts were found. The body lay in a supine position, aligned approximately west/east but with the legs extended in a north-east/south-west direction. The left arm was flexed at the elbow so that the forearm lay across the pelvis. The right arm seems to have been disturbed and the skull was also missing.49 A number of pathological features were noted, including some degenerative joint disease on the shoulder and vertebrae. A sample of the human remains was submitted for radiocarbon dating and yielded a date of 1405±40 BP, which calibrates to 569–675.50
Grave 2
This underlay grave 1 and consisted of a lintel grave, rectangular in plan, aligned east/west. Internally it measured 2.33m long by 0.4m wide (Fig. 4.24).51 The cist tapered slightly in width from 0.4m at the east to 0.28m at the west. It was formed of ten slabs set on edge, four remaining on the northern side, three on the southern and one closing the western end.
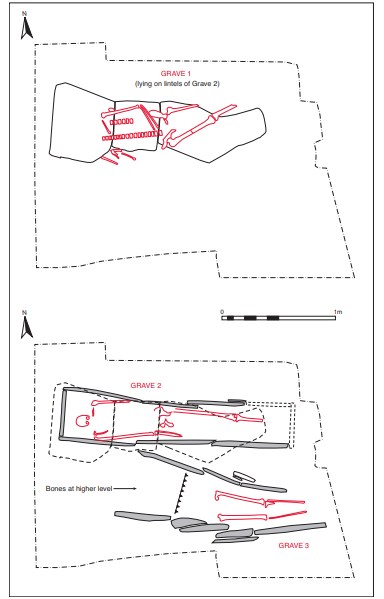
It is probable that there was originally a fifth side slab at the northern side and also a closing slab at the eastern end. The maximum thickness of the slabs was 0.05m and maximum length 0.66m. The cist was not paved but was covered with three large lintels, the longest measuring 0.94m. There was no evidence for packing stones or for the pit dug to receive the cist.
The cist contained a well-preserved inhumation, also of an older adult male (1958:167), again without any accompanying artefacts. The body lay extended in a supine position with the arms by the sides, legs extended and the skull to the west. Traces of degenerative joint disease, vertebral joint disease and diffuse idiopathic skeletal hyperostosis (DISH) were noted on this skeleton by Buckley (see below). A sample of the human remains was submitted for radiocarbon dating and yielded a date of 1490±45 BP, which calibrates to 435–649.52
Grave 3
Immediately south of grave 2, a line of thin edge-set slabs was revealed, similar to the side slabs of grave 2 (Fig. 4.24). These were excavated and found to comprise the northern side of a second cist. Although lacking end slabs, this cist was roughly rectangular in shape and was aligned west/east. The remaining length of the cist was in excess of 1.8m. Its maximum width was 0.48m (near the western end), tapering to 0.4m near the eastern end.53 The sides of the cist comprised nine slabs in total, three on the northern side and six on the south, many of which overlapped, giving the appearance of a double row of slabs in some places. The cist was not paved and there was no evidence for lintels or covering slabs in the vicinity. There is no evidence in the site records that excavation revealed packing stones or the pit dug to receive the cist. This cist may originally have been covered with lintels that were disturbed prior to Ó Ríordáin’s investigation, but Ó Ríordáin does not comment on this possibility.
The grave contained the disturbed remains of an adult male (1958:166) aged 25–34 years at death. Some of the bone in the grave had been disturbed, and the femora and tibiae lay extended (apparently in situ) 0.17m lower than the bone at the western end, which was disarticulated. The excavator suggested that the bone at the western end represented a later burial in this grave, although Buckley only found that the remains represented a single individual. Buckley has noted a large number of sharp cuts to the vertebrae, ribs, pelvis and legs of the individual, which indicate that the individual may have been tortured before being killed. The cuts on the cervical vertebra may indicate decapitation around the time of death (see below). A sample of the human remains was submitted for radiocarbon dating and yielded a date of 1420±45 BP, which calibrates to 553–670.54
Comment
Analysis of the skeletal remains showed that this cemetery contained a mixed population, with adult males and females as well as juveniles and infants represented. Evidence for diffuse idiopathic skeletal hyperostosis (DISH)—a disease associated with rich diets and often found on monastic cemetery sites—on one of the skeletons indicated that this individual may be of high status (see Buckley, below). This site does not appear to be associated with a church site, and it may be an ancestral burial ground that remained in use until at least the seventh century.
HUMAN REMAINS
LAUREEN BUCKLEY
Skeleton 1 (grave 1): older adult male, 172cm (1958:165)
This supine, extended burial was found lying over the lintels of the grave below. It was in a good state of preservation but the skull and most of the lower legs and feet were missing. None of the missing bones were found with the miscellaneous bone from the site, but the bone in the left lower leg position on the plan was a femur from a female skeleton. There were other parts of a female skeleton present and the description of these is dealt with under the miscellaneous bones.
The skull and cervical vertebrae were missing, but the thoracic and lumbar vertebrae were present and all were complete, apart from the first thoracic vertebra. There were six ribs from the left side and three from the right side present.
The left scapula was present and the left clavicle was complete, apart from the lateral end. All the bones from the left arm, humerus, radius and ulna, were complete. Only a fragment of acromion from the scapula, the distal half of the right humerus and the complete right ulna remained from the right arm. The lunate, triquetral, capitate and hamate, five metacarpals and one proximal phalanx remained from the left hand. The right hand consisted of the scaphoid and hamate, all the metacarpals apart from the first, five proximal phalanges and one middle phalanx.
Both the ilia, the ischia and the pubic bones were present from the pelvis but they were not complete. Only the first sacral vertebra survived. The proximal two-thirds portion of the left femur was present and the right femur was complete. The proximal halves of the right tibia and fibula were also present.
Age and sex
All the observable features of the pelvis—the sub-pubic concavity, sub-pubic angle, ischiopubic ramus ridge and sciatic notch—were of the male type. The diameters of the heads of the femurs, humerus and radius and the femoral bicondylar width were all in the male
range.
The auricular surface of the ilium and the pubic symphysis surface indicated that this was an older adult, at least over 50 years of age. Stature was estimated, using the length of the femur, as 172cm.
Skeletal pathology
Anomalies: there were six lumbar vertebrae instead of the usual five and eleven thoracic instead of twelve.
Degenerative joint disease: there was some degeneration of the left shoulder joint, with mild marginal lipping and slight porosity of the head of the humerus and porosity of the lateral surface of the clavicle. At the right elbow there was porosity of the radial surface on the proximal ulna. Both hip joints had evidence of DJD, with surface osteophytes on the superior part of the acetabula and slight marginal lipping. The right side was more affected than the left.
Vertebrae: degenerative joint disease was present throughout the vertebral column, with moderate to severe lipping and porosity of most articular surfaces of the upper six thoracic vertebrae and the lower two thoracic vertebrae. There was mild degenerative joint disease in the lumbar vertebrae. Osteophytosis affected the middle thoracic vertebrae to a mild degree and was moderate to severe in the lower thoracic vertebrae. There was also mild osteophytosis in the upper and lower lumbar vertebrae, with the middle lumbar being affected to a moderate degree. Degenerative joint disease was also present to a mild degree in the upper and lower costo-vertebral joints. Schmorl’s nodes affected the lower thoracic and upper two lumbar vertebrae.
Other pathology
There were small enthesophytes on the lesser tuberosity of the left humerus.
Additional bones
The bone in the left lower position drawn in the plan of this skeleton is actually a femur from a female skeleton. There were other female bones present also and these are described in the miscellaneous section.
Skeleton 2 (grave 2): older adult male, 177cm (1958:167)
This supine extended skeleton lay in a stone-lined cist with a lintel covering and was virtually complete, apart from the right femur. The skull was complete, apart from the right side of the maxilla and part of the left side. The upper three cervical vertebrae were complete and fragments of the fourth and fifth were also present. The upper thoracic vertebrae were missing but the lower seven were complete and the neural arch of the first lumbar vertebra was also present. Nine ribs from the left side and ten from the right were present and the body of the sternum was complete.
Both scapulae were virtually complete. The lateral end of the left clavicle was present and the medial end was missing from the right clavicle. All the arm bones were complete. Only the left hamate remained from the carpal bones, but all the left metacarpals and the right second, third and fourth metacarpals were complete. Three proximal phalanges from the right hand were present.
Both ilia were present but incomplete, part of the left ischium survived and the right ischium was complete. Most of the sacrum was present. The left femur, left patella and both tibiae were complete and the proximal two-thirds of the left fibula was also present. There were no foot bones remaining.
Age and sex
The sciatic notches in the pelvis were narrow, indicating that this was a male individual. All the features of the skull, the external occipital protuberance, the mastoid processes, the supraorbital ridges, the orbital rims and mental eminence of the mandible, were of the male type. The diameters of the heads of the femurs, humeri and radius as well as the bicondylar width of the femurs and the glenoid cavity widths were all in the male range. The auricular surfaces of the ilia were not visible and there were no pubic bones. The only method of ageing was the teeth and the skull sutures. The teeth were heavily worn, suggesting an older adult, and the skull sutures were almost obliterated, again suggesting an older adult. The living stature was estimated, using the lengths of the femur and tibia, as 177cm.
Non-metric traits
The metopic suture was retained. There was a third trochanter on the left femur, a vastus notch on the left patella and a squatting facet on the right tibia.
Skeletal pathology
Cribra orbitalia was present to a moderate degree in the right orbit and to a mild degree in the left orbit.
There was a healed fracture on the left third metacarpal. The broken ends of the bones had overlapped considerably but the fracture is well healed and the callus was very smooth (Pl. 111).
Degenerative joint disease
DJD affected both shoulder joints. There was moderate marginal lipping around the inferior half of the left glenoid fossa and moderate porosity of the acromial end of the clavicle. The head of the humerus had mild to moderate marginal lipping, with slight porosity of the most superior part of the surface. At the right shoulder there were severe marginal osteophytes around the head of the humerus, especially on the anterior and inferior edges, moderate lipping around the glenoid fossa of the scapula and severe porosity of the acromial facet of the scapula and lateral end of the clavicle.
At the left elbow there was mild marginal lipping of the lateral edge of the trochlea on the humerus and also the lateral edge of the capitulum. There was also mild lipping all around the proximal joint surface of the ulna. The right elbow was difficult to examine since the distal end of the humerus was encrusted in a mineral deposit, but there appeared to be slight marginal lipping around the trochlea and around the inferior and lateral edges of the capitulum. There was also moderate lipping around the proximal articular surface of the right ulna. There was moderate lipping around the distal end of the right ulna but there were no right carpal bones of the wrist present to examine.
At the hip joints there was mild marginal lipping and surface osteophytes on the superior part of the left acetabulum and very mild lipping on the superior part of the right acetabulum. Both acetabula have an ossified shelf of bone on the inferior margin, which is probably a ligament ossification. Mild lipping was also present at the head of the left femur. There was moderate lipping all around the medial condyle of the left femur and the medial edge of the lateral condyle. There was also mild lipping around the medial condyle on the left tibia and on the left patella.
Vertebral joint disease
Osteoarthritis was present in the cervical vertebrae, with eburnation of the joint surfaces on the left side between C2 and C3. There were mild degenerative changes on the joints on the right side. In the mid-thoracic vertebrae there were mild to moderate degenerative changes in the posterior articular surfaces from T5 to T9.
Osteophytosis was present to a moderate degree in the sixth thoracic vertebra but was severe in the lower thoracic vertebrae, T7–T12. The left side of the body of the seventh thoracic vertebra was slightly compressed. The tenth and eleventh thoracic vertebrae were fused by the large osteophytes on the anterior and right sides of the vertebral bodies. This is described in more detail under DISH, below.
Schmorl’s nodes were present on the inferior surfaces of T5–T7, the superior and inferior surfaces of T8 and T9, the superior surface of T10, the inferior surface of T11 and both the superior and inferior surfaces of T12. The inferior surface of T10 and the superior surface of T11 were not observable as the vertebrae were fused. All the Schmorl’s nodes were very deep and Irregular.
Diffuse idiopathic skeletal hyperostosis (DISH)
The lower thoracic vertebrae T10 and T11 had completely fused together and, although they were now separate, it is possible that T12 and L1 may also have been fused during life. In addition, some of the costal cartilages had ossified and the fourth ribs on each side were fused to the sternum, with the third and fifth ribs having begun to fuse. The tenth and eleventh thoracic vertebrae were fused by a solid osteophyte on the anterior and right side of the vertebral bodies only. This osteophyte was smooth and had the appearance of ‘dripping candle wax’. The posterior vertebral joints were unfused and the vertebral disc space was maintained. The eighth thoracic vertebra also had a large osteophyte on the right side of its body, which had the ‘dripping candle wax’ appearance (Pl. 116).
Fusion of at least four continuous vertebrae as described above, along with fusion of the ribs, is typical of a condition known as diffuse idiopathic skeletal hyperostosis (DISH). In this condition osteophytes form only on the right side of the middle thoracic vertebrae, such as is present in T8 and T9, as the descending aorta prevents ossification on the left side. In the lower thoracic and lumbar, fusion can occur on the anterior surface. It is unfortunate that most of the middle and upper thoracic vertebrae are missing in this individual.
Fusion of the ilia to the sacrum by ossification of the superior ligament has occurred on both sides. The joint surface is not affected and the joint space is maintained. This is another feature of DISH, although it is not present in all cases. It is easily differentiated from ankylosing spondylitis (AS), another condition where the pelvis can fuse, as in AS degeneration of the articular surface of the ilium occurs and fusion occurs across the joint surface.
Another feature of DISH is the development of enthesophytes (ligament ossifications) on extraspinal bones. In this individual enthesophytes were present on several bones. The linea aspera of the left femur was very well developed and the greater trochanter had a very rugged appearance owing to enthesophytes. There was also a well-developed soleal line on the left tibia, and the insertion for quadriceps femoris on the left patella was very pronounced. On the right tibia the soleal line was a smooth ridge of bone, suggesting that there may have been some traumatic damage to the ligaments attaching the soleus muscle that resulted in a bony reaction.
The greater and lesser tuberosities of the left humerus were rugged and porotic and the lesser tuberosity of the right humerus was very rugged. There was also a very strong attachment for the triceps brachii muscle at the olecranon of the right ulna.
Three ribs from each side have well-ossified ligament attachments at the tubercles. One from the left side has a large ligament ossification at its head.
In the thoracic vertebrae, particularly the fifth thoracic, there is a build-up of bone in the superior parts of the arches between the superior articular surfaces. This represents ossification of the ligamenta flava, which connect adjacent vertebrae at the laminae and are important in the flexibility of the spine.
The cause of DISH is uncertain, but males are usually more affected than females and the usual age of onset is over 50 years. It has been found in high proportions in monastic cemetery sites (Stroud and Kemp 1993; Waldron 1985), and there is thought to be some association with obesity and mature-onset diabetes. It has also been suggested, however, that some individuals are ‘bone-formers’ and that ossification may result from an exaggerated response to stimuli in some people when similar stimuli would produce a modest response in others (Resnick and Niawayama 1988).
It seems likely that this individual was a bone-former, as the fractured metacarpal is very well healed and there is a significant degree of ligament ossification. Nevertheless, it is also likely that this person was very well nourished and possibly of high status. His estimated living stature of 177cm is well above that normally found in past populations and is above the average stature found in modern populations.
Dentition
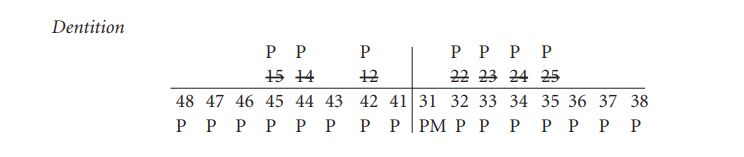
Attrition: there was very heavy attrition on the upper teeth. In fact, they were so badly worn that it was difficult to identify them. There was also heavy wear on the lower incisors, with moderate wear on the canines and premolars. Attrition was extremely heavy on the lower first and second molars but light on the third molars.
Calculus: there were moderate deposits on the lingual surfaces of the right mandibular teeth and light deposits on the lingual and buccal surfaces of the left mandibular teeth. Calculus deposits were also visible on all exposed roots.
Periodontal disease: there was considerable recession of the sockets of all teeth in the mandible.
Skeleton 3 (grave 3): early middle adult male, 165cm (1958:166)
This skeleton was contained in a long cist aligned west/east. It was supine and extended and was almost complete, apart from the skull, left lower arm and pelvis. The cist had no remaining covering and the bones at the upper end of the grave seem to have been disturbed. The vertebral column consisted of the partial remains of the upper two cervical vertebrae, the arch of the fourth cervical vertebra, the lower three cervical vertebrae, all the thoracic vertebrae and the upper two lumbar vertebrae. There were eight ribs from the left side and nine from the right side remaining.
The clavicles were complete and the scapulae were virtually complete. Both humeri and the right radius and ulna were complete but the left radius and ulna were missing. The left hand was also missing but all the carpals of the right hand apart from the trapezoid were present, along with the third, fourth and fifth metacarpals and five proximal and two middle hand phalanges.
Although the pelvis was missing, a right ilium from the miscellaneous bones appeared to belong to this skeleton. Both femurs and the right tibia and fibula from the leg bones were complete. The left fibula was complete but only the proximal end of the left tibia was present, although the distal half of the tibia was found among the miscellaneous bone. Only the talus, calcaneum, navicular and first cuneiform as well as the first metatarsal remained from the left foot. The right foot consisted of all the tarsals apart from the third cuneiform as well as the first three metatarsals.
Age and sex
The sciatic notch was of the male type. All the metrical analysis, diameter of the femoral and humeral heads, femoral bicondylar width and glenoid fossa width were in the male range. The auricular surface of the ilium and the sternal ends of the ribs indicated that this was an early middle adult aged 25–34 years.
The estimated living stature, calculated using the lengths of the femur and fibula, was 165cm.
Skeletal pathology
The most startling skeletal pathology present was the large number of sharp cuts to the vertebrae, ribs, pelvis and legs of this individual.
Vertebrae: only the neural arch of the fourth cervical vertebra was present, but it had a straight cut through the right side just below the superior articular surfaces. There was a sharp edge to the cut, which had gone smoothly through the bone. Most of the left side of the arch was missing below this level. Although most of the vertebra was missing, it is probable that this cut represents a decapitation, since a cut through the thin lower cervical vertebrae is the most efficient and most common method of decapitation. The skull of this burial was missing so it is unlikely to have been buried with the rest of the body. If decapitation did occur, it is unlikely that the fragments of the first and second cervical vertebrae that were present belong to this individual. As there was disturbance to the upper part of the skeleton, however, it is more than probable that these fragments do not belong to this individual. The first thoracic vertebra has a small linear cut on the back of the neural arch also on the right side at the inferior edge near the articular surfaces.
The first lumbar vertebra had an oblique cut on the anterior surface of the vertebral body.
Left ribs: several ribs from both sides had evidence of cut-marks. On the left side the first rib had five tiny cut-marks on the anterior edge, all approximately 4mm long and 7mm apart. At least six of the other ribs had several cuts near their heads and necks, close to where they would have articulated with the vertebrae at the back of the body. Three of these ribs have only a few cuts visible but there are more extensive cuts on the others, some on the inferior and superior edges as well as a few on the internal surface of the rib. Most of the cuts follow the same basic pattern, consisting of small, incised lines, but occasionally a diagonal or even horizontal cut was present, with these cuts being larger than the rest. In some instances bone was sheared off from around the larger cuts. One rib in particular had a large slice sheared off its superior surface. In a few places the cutting instrument, possibly a knife, had entered at a slight angle, producing a V-shaped cut. There were also a few cuts on the external surface of the ribs but these tended to be shallower than the others, apart from one near the sternal end of the rib, which had an oblique cut that almost went all the way through the bone. One small cut on the inferior edge of a rib had been delivered with such force that it had fractured the bone.
Right ribs: at least seven ribs from the right side also had cuts, but there were not as many and they were not as severe as on the left side. Most of these cuts were on the internal and inferior surfaces, although there was one on the external surface. Most of the cuts were short and shallow.
Clavicles: the left clavicle had several small, incised cut-marks on the posterior surface and superior edge. In the medial half of the bone there were two small cuts, 3.5mm and 4.5mm long and 2cm apart. The lateral half of the bone also had two cuts 9mm apart and there were also a few tiny cuts. The right clavicle had four small, incised cuts on the posterior surface in the lateral half of the bone and also some tiny nicks near the medial end.
Scapulae: the left scapula had no obvious lesions, but on the right scapula there was a small cut on the posterior surface just below the acromial spine.
Left femur: the left femur had a small cut on the medial surface in the middle of the shaft.
Right femur: the right femur had some shallow, sharp, incised cuts on the anterior surface just below the neck. There was a cut, 13mm long, on the medial border at the level of the lesser trochanter, which was almost vertical and appeared to have occurred from the lower end upwards. At the most inferior edge of the cut the bone was smooth and ended in a sharp line, with the upper end being roughly broken off. There were also several cuts on the lateral border with sharp incised lines on the proximal half of the bone. Some were slightly elongated and slightly sheared off. On the posterior surface in the proximal third of the bone there were at least four cuts, which were sharp, incised but shallow. In addition, on the lateral surface of the femur there were a series of small perforations, 2mm in diameter, up the entire shaft. It is not known what could have caused these holes.
Right tibia: there was a sharp, incised, shallow cut, 26mm long, on the lateral surface near the proximal end. There was another cut 9cm below this one, also on the lateral surface, also shallow and of the same length.
Right pelvis: the internal surface of the ilium, the iliac fossa, has four diamond-shaped perforations, with a maximum length of 3–6mm. There was some slight shearing around the edge of one of the wounds.
It is very difficult to interpret the wounds on this skeleton. The cut to the fourth cervical vertebra probably caused decapitation, although as the vertebra is incomplete this cannot be certain. There were some cuts to the back of the ribs but most of the cuts were on the internal surfaces and on the superior and inferior edges of the ribs, almost as if someone was trying to cut between the ribs. The rib cage is a very efficient protection device for the heart and lungs. It would be difficult by a direct blow to the front of the body to hit the heart. One rib from this individual had a cut on the front surface near the sternal end which must have been delivered with some force but which had not managed to cut through the bone. Obviously the most efficient way of killing someone with a knife is to stab them below the sternum, aiming the blade up and under the ribs to penetrate the vital organs of heart and lungs. This method, if applied with enough force, could cause cut-marks on the internal surfaces of the ribs such as is seen here. But why were there so many of them? Could it be that this person was cut after death to remove internal organs?
The cuts on the external surfaces of the ribs were very shallow and barely cut the surface of the bone. There were also shallow cuts on the back of the clavicles and scapula and on the front and back of the femurs, as well as the outside edge of the bone. The lower leg also had some cuts on the outside edge.
The cuts on this person do not seem consistent with a fair fight, one opponent facing another and both able to defend themselves with the same weapons. There are so many wounds on this man that it is possible that he was tortured before death. An instrument that cut flesh but barely cut the bone surface must have caused the shallow incised cuts on the outer surfaces of the bones. The perforations on the inside of the ilium appear to have been caused by an instrument or weapon with a diamond-shaped profile. At the present time it is not possible to speculate on what type of weapon this could be. Again, they do not seem to have been caused in battle, as it would be very difficult to penetrate the inner surface of the ilium while an individual is upright and capable of defence. These were probably caused at or around the time of death while the man was in a supine position.
Other pathology
The left humerus was slightly encrusted with mineral deposits but there was evidence of slight degenerative joint disease at the shoulder, with mild marginal lipping and slight surface porosity of the proximal humerus surface.
Slight DJD was present in the upper and middle thoracic vertebrae, with mild lipping of some of the posterior articular surfaces.
There was a small area of healed osteochondritis on the proximal right ulna, in the most superior part of the joint.
There were very deep Schmorl’s nodes on the inferior surface of the first lumbar vertebra and a crescent-shaped area of erosion near the anterior border. Schmorl’s nodes were also on the superior surface and on the superior and inferior surfaces of L2, where they were very deep. Very deep Schmorl’s nodes were present on the lower thoracic vertebrae T7–T12.
Miscellaneous bone
Adult long bones
Clavicles: two right clavicles were present, one with the medial end missing and one consisting of a decayed shaft only.
Scapulae: there was one right scapula with most of the glenoid fossa and acromion present as well as the lateral border.
Sternum: one part of the body of a sternum.
Humerus: one almost complete left humerus, but the proximal end was missing.
One virtually complete right humerus with the proximal end missing, probably a match of the left humerus.
One almost complete right humerus but the head was missing.
The proximal two-thirds of a right humerus and a distal joint end, which may have belonged to the same bone.
Radius: one left radius, almost complete, but the head was missing. The bone was small and slight and may have been from a female.
There were four right radii. One consisted of the distal two-thirds and the other three consisted of the proximal halves of the bones only.
Ulna: there were two left ulnae; one consisted of the proximal two-thirds of the bone and the other consisted of the proximal half.
There were also two right ulnae; one was almost complete but the distal end was missing, and the other was complete (UlL1 231mm).
Femur: there were four left femurs; three were complete and appeared to be from female individuals.
(FeL1 425mm, FeHd 42.3mm, FeE1 76.0)
(FeL1 394mm, FeHd 40.3mm, FeE1 69.2mm)
(FeL1 393mm, FeHd 39.6mm, FeE1 71.1mm)
The other one was almost complete but the head and neck were missing.
There were three right femurs. One was complete and appeared to be from a female; it also appeared to be a match for one of the right femurs.
(FeL1 394mm, FeHd 39.5mm, FeE1 71.3mm)
One was almost complete with only the head and neck missing, and one was missing its proximal third.
Patella: there was one right patella present.
Tibia: three left tibiae were present. One was complete, one consisted of the proximal twothirds, although there was also a distal end that might have belonged to this bone, and one consisted of the proximal half. (TiL1 340mm, TiE1 71.2mm)
A minimum of four right tibiae were present. One was complete (TiL1 321mm, TiE1 61.0mm), one consisted of a proximal third, one consisted of a proximal two-thirds and the other was a proximal end only. There was also a distal half of a right tibia and a distal end that could have belonged to these bones.
Fibula: the distal ends of a left and a right bone were present, as well as the proximal third of a right bone and fragments from two shafts.
Pelvis: two left and three right innominates were present. One of the left, consisting of an ilium and ischium, was probably from a male as the sciatic notch was narrow. The auricular surface of the ilium suggested that he was an early middle adult. The other left innominate, also consisting of an ilium and ischium, had a wide sciatic notch so was probably female. It was from an older adult.
One of the right innominates, consisting of an ilium only, was from an older adult female. There was another ilium and ischium from a middle adult female, and the other innominate consisted of a right acetabulum and part of the ischium only.
Sacrum: there were two sacra present. One consisted of the upper three sacral vertebrae and was from a female; the other consisted of two sacral vertebrae only but may also have been from a female.
Vertebrae: three lower lumbar vertebrae were present, L3–L5, as well as the neural arch of a first lumbar vertebra. A complete first thoracic and the arch of another first thoracic were present, as well as the body of another thoracic vertebra and another complete upper thoracic vertebra.
One complete atlas was also present.
Schmorl’s nodes were present in the superior part of L3.
Ribs: two left ribs, including a first rib, were present, and there was one right rib.
Foot bones: these included two left calcanea, the posterior half of a right calcaneum, two left and one right tali, one right first metatarsal, one right second metatarsal and the shaft of one other.
Hand bones: only a left second metacarpal remained
Adult skull bones
(1) This consisted of a complete skull and mandible. The cranium was intact and in one piece with virtually all bones present. All the sutures were well fused so it was probably an old adult, and all the morphological features of the skull indicate that it was a female.
Dentition:
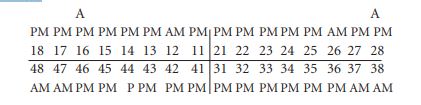
Antemortem loss: at least six teeth had been lost during life. This was probably a result of old age and the considerable recession of the alveolus. Five of the lost teeth were molars and one was the upper right lateral incisor. All of the remaining molars had very shallow roots, suggesting that they were on the point of being lost at the time of death. Abscesses: there was an abscess at the buccal root of the upper right first molar, 16, which opened internally into the maxillary sinus. There was also an external abscess at the buccal root of the upper left third molar.
Other skull bones
There were a number of other skull bones present. These included a matching left and right parietal bone, another left and right parietal bone possibly from the one individual, the orbital areas of a left and a right frontal bone and a minimum of three adult occipital bones. Two left and three right sides of mandibles were also present, as well as two left and two right maxillae.
Left and right nasal bones were also present.
Mandible 1

Attrition: there was heavy wear on the right first molar and moderate wear on the other teeth.
Calculus: there were moderate deposits on the buccal surfaces of all the teeth on the right side and on the lingual surfaces of the right first and second molar. Deposits were heavy on the lingual surfaces of the right premolars.
Periodontal disease: there was slight recession around the roots of the premolars and molars.
Mandible 2
The bone of the mandible and some of the roots of the teeth were very decayed. There was moderate attrition on the first molar and premolar and light wear on the other teeth. Linear enamel hypoplasia was noted on the premolar and first molars.
Mandible 3

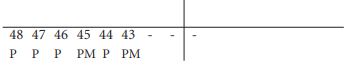
This seemed to be a male-type mandible, with a square mental eminence and flared gonial region.
Abrasion: there were chips out of the enamel of the mesial/lingual corners of the first molar and second premolar, 35 and 36. This had occurred during life as some calculus had been deposited in the gaps.
Attrition: there was moderate wear on the first molar and light wear on the other teeth.
Calculus: there were moderate deposits on the occlusal surface of the first premolar.
Maxilla 1

Attrition: there was moderate wear on the remaining teeth.
Calculus: there were light deposits on the buccal and lingual surfaces of the left first molar.
Hypoplasia: linear enamel hypoplasia was present on the premolars and right first molar.
Maxilla 2
Attrition: there was heavy wear on the right first molar and moderate wear on the remaining teeth.
Calculus: there were light deposits on the distal surface of the left first molar and buccal surface of the left second premolar. Deposits were moderate on the buccal surfaces of the teeth in the right side of the maxilla and on the buccal surface of the left incisor. Deposits were considerable on the lingual surfaces of the right first molar.
Periodontal disease: there was a slight degree of recession around most teeth on the right side and moderate recession around the roots of the left premolar and first molar.
Hypoplasia: linear enamel hypoplasia was present on the left lateral incisor.
Table 4.5—Summary of identified bones, 1958:168.
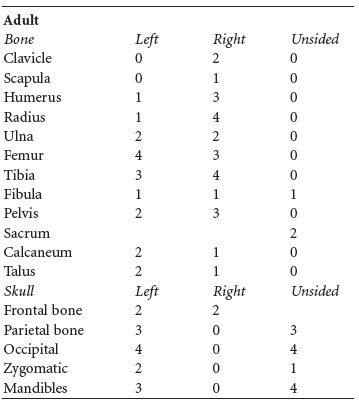
The minimum number of adult individuals is therefore four, based on the number of occipital, mandible, tibia and radius bones. Since all three burials had their right tibiae present, these disarticulated bones represent the remains of an additional four adults.
Juvenile bones
The juvenile bones could be divided by size into older juvenile, younger juvenile and infant. Older juvenile: these bones included a section from the mid-shaft of a right femur, a section of left tibia shaft, the proximal half of an ulna, a complete left ilium, part of a right ilium, both with unfused acetabulum, a right ischium and a first sacral vertebra.
Also present was an occipital bone and a left temporal bone from an older juvenile or adolescent.
Younger juvenile: this consisted of a left ilium, as well as an additional juvenile ulna found with skeleton 2.
Infant: these included a virtually complete left femur (79mm), a complete right tibia (70mm), the proximal half of a left tibia and a petrous temporal bone from the skull. These bones could have come from the one infant, which from an estimation of the body length was more than full-term so was probably not a neonate. From the size of the bones, however, it is unlikely that the infant was more than a few months old.
Summary
The remains from this site consisted of three adult males, with an additional four adults, two juveniles and one infant found in the disarticulated bones. One of the burials lay over a lintel grave, one was in the lintel grave and the other was in a slab-lined grave that may have been a disturbed lintel grave. Two of the burials were older adult males and the one in the slab-lined grave was an early middle adult male, aged 25–34 years at the time of death. The four disarticulated adults appeared to represent at least three females and one male. The dentition of the individuals had the typical heavy wear and calculus seen in earlier populations and also a complete lack of caries. This indicates that they were probably medieval or earlier burials. Both older adults, not surprisingly, had evidence of degenerative joint disease. Burial 1 had degenerative disease of the spine, left shoulder, right elbow and both hips. Burial 2 had both shoulders, both elbows, both hips and the left knee affected. The spine was very badly affected with osteoarthritis of the cervical spine, a compressed middle thoracic vertebra and deep, irregular Schmorl’s nodes.
Burial 2 was also affected by another condition, known as diffuse idiopathic skeletal hyperostosis (DISH). Ossification of the costal cartilages had occurred, with ribs fused to sternum and the lower thoracic and first lumbar vertebrae fused together. There were large osteophytes on the right side of the middle thoracic vertebrae that had the appearance of ‘dripping candle wax’. Fusion of the ilia to both sides of the sacrum without affecting the joint surfaces had also occurred. There were also several examples of enthesophytes, calcification of ligament insertions, on various bones. These are all features of DISH. The cause of DISH is uncertain but there seems to be some link with mature-onset diabetes and a rich diet. It has been found frequently on priory sites in England where individuals of high status have been buried and is increasingly being recognised in Irish skeletal material, particularly on individuals from high-status graves or sites (Buckley 2002; Halpin and Buckley 1995). This individual could be deemed to be high-status since he was in a well-made lintel-covered grave. It is also thought, however, that some individuals form bone more easily than others and can therefore develop this condition. It seems likely that this individual was a bone-former as he had a very well-healed fractured metacarpal and a significant degree of ligament ossification. It is also likely that this person was very well nourished and so of high status. His estimated living stature of 177cm is well above that normally found in past populations and above the average stature found in modern populations, suggesting that he did not suffer from malnutrition while he was growing. The early middle adult male was also very interesting. He had suffered a number of cuts to the neck, back, ribs and legs, and had unusual wounds on the pelvis and femur. It is
probable that this man was beheaded but it was also possible that he was tortured before being killed, and may even have had internal organs removed.
Conclusions
The human remains from this site represent the remains of seven individuals. The remains indicate a mixed population, comprising males, females and juveniles. It is probable that the cemetery was of substantial size—only a small area was excavated by Ó Ríordáin. The cemetery does not appear to have been directly associated with a church.
48. Parish of Killashee, barony of Naas North. SMR KD024-018——. The exact location of the site has not been marked.
49. A skull reportedly found just outside the grave may belong to this burial.
50. GrA-24582.
51. The height of the cist is not known.
52. GrA-24583.
53. The height of the cist was not recorded.
54. GrA-24503.